Leslie Upledger Ray, MA, MPPA; Alan M. Smith, MPH; Dale L. Cooper; Patti M. Akers, MA; Patricia A. Murrin, RN, MPH
Medical emergencies such as flu outbreaks pose significant challenges to emergency medical and hospital resources. This paper examines the impact of a major influenza outbreak on paramedic/EMT and emergency department resources on a major metropolitan area. Population density, travel time, topography and medical resources were analyzed. This paper discusses the development of a predictive model for resource allocation in the event of a future outbreak.
Emergency department diversion is a critical problem in emergency health care nationwide. When an emergency department goes on diversion paramedics transporting patients are diverted to the next available hospital. This increases the transport time for the patients and the amount of time the paramedic unit is unavailable for other calls. Diversion can also create a domino effect when the overflow from one hospital causes another to go on diversion and so on. While emergency departments typically handle patient volume without incident, unusual occurrences such as flu outbreaks can stress the system to the breaking point.
We began to examine patterns in emergency department utilization after the 99/00 flu season brought available resources to critically low levels. In an effort to avert future resource problems, we needed to develop a model for predicting need by patient location and by resource location.
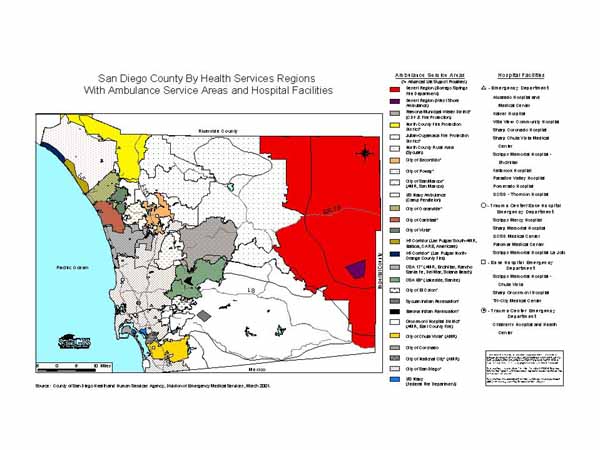
San Diego County has over two dozen ambulance service areas manned by 47 first responder agencies, 20 emergency departments, and six trauma centers. In the last two years, two emergency departments have closed.
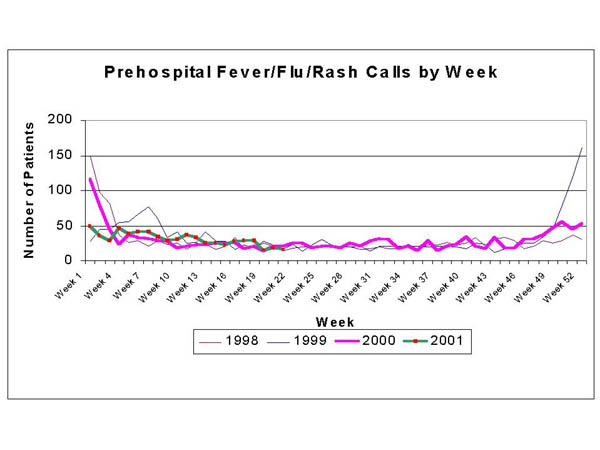
Data from the County of San Diego Division of Emergency Medical Services' QANet system was analyzed for this study. Prehospital data from the base hospitals as well as hospital bypass data was included. Historical data from the previous four years was reviewed for trends. Prehospital patients with a chief complaint of fever/flu/rash were analyzed. A weekly plot of cases was produced to identify flu outbreak time periods. Age and location specific population data including projections were obtained from the San Diego Association of Governments (SANDAG). Distances and travel times were calculated using base maps from SANGIS and ArcView 3.2 software.
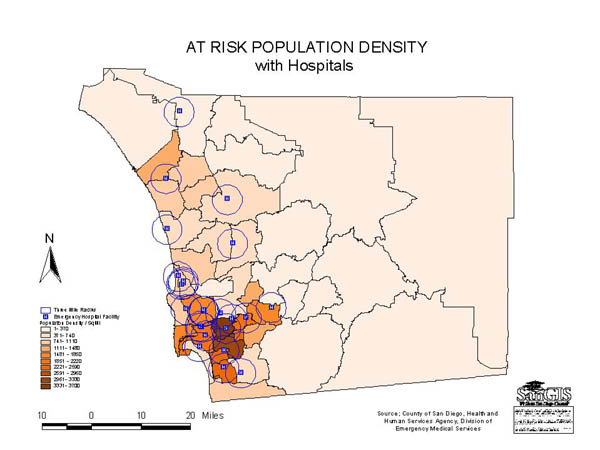
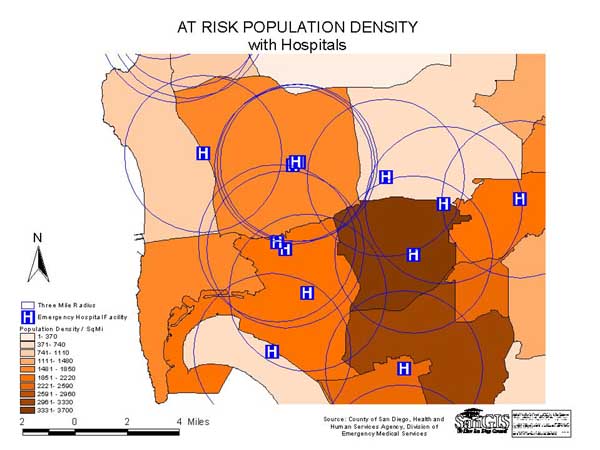
Population densities were calculated for subregional areas (SRAs) based on numbers of high risk individuals per square mile and converted to dBase format. High risk was defined as under age 15 and over age 64 or resident of a care facility in accordance with definitions established by the Centers for Disease Control and Prevention. A chloropleth map was created to show the SRAs with the highest potential need for transport due to flu symptoms. This map was layered with locations of emergency departments and mileage to demonstrate the available resources within SRAs with greatest potential need. All mapping was performed using ArcView 3.2. The mathematical model was built using Microsoft Excel.
An analysis of the full years of prehospital data from 1998-2000 showed that paramedics typically responded to flu 30 calls per week during normal weeks and as many as 160 calls during flu season weeks. Annually there were 1491, 1792 and 1564 calls respectively. Between 12/26/99 and 1/7/00, the 99/00 flu outbreak, the 21 hospitals were on bypass due to emergency department saturation a total of 3300 hours out of a possible 6552, or an average of 157 hours out of a possible 312 hours per hospital. Emergency departments go on diversion for a variety of reasons, but essentially it is because they do not have staff and/or facilities to treat additional patients.
The model was created to assess the available resources in each emergency department, projected background rate of other prehospital patient activity, potential patients at risk for the medical emergency and distance/time between facilities and at risk population locations.
Combining population health surveillance techniques and demographic projection methods with GIS allows for the development of a predictive model for emergency medical resource allocation. While software and algorithms have been developed to project spread of infectious or biologic agents and also for resource distribution, our task was to combine these methodologies into a single model that would allow for the identification of populations at risk, predict the potential number of patients impacting resources, identify the emergency medical resources available and match projected needs to resources. The key component of this model was the ability to identify the locations of high risk patients compared to the general population.
While we used flu as the medical emergency in this example, the model can be adjusted for other medical and injury emergencies that occur over several days. It is not appropriate for single events such as multiple victim motor vehicle crashes that are resolved using emergency triage protocols already in place.
Managed care restrictions are a complicating factor for both self-transported patients and those transported by emergency medical personnel. By requiring patients to go to specific emergency departments within their plans, managed care organizations control their costs. However, the emergency department that is part of the patient's plan may not be the closest geographically. This could seriously impact the model by changing the predicted pattern of emergency department use by self-transport patients thereby impacting available resources for available transported patients. This will require further research with prospective data collected during the next medical emergency.
Leslie Upledger Ray, Senior Epidemiologist, email lrayxxhe@co.san-diego.ca.us
County of San Diego, Health and Human Services Agency, Division of Emergency Medical Services, 6255 Mission Gorge Rd, San Diego, CA 92120, phone: 619.285.6429, fax: 619.285.6531